


Contents
Scroll to:
 A. M. Wibisono,
A. Fauzi,
D. Friska,
K. A. Suryoadji,
M. Abdullah,
D. G. Sudrajat,
A. Surandy,
V. N. Muzelina,
A. F. Syam
A. M. Wibisono,
A. Fauzi,
D. Friska,
K. A. Suryoadji,
M. Abdullah,
D. G. Sudrajat,
A. Surandy,
V. N. Muzelina,
A. F. Syam https://doi.org/10.47093/3034-4700.2025.2.2.46-51
Scroll to:
Background: Reverse transcription polymerase chain reaction (RT-PCR) using lower gastrointestinal (GI) specimens can detect SARS-CoV-2 RNA in patients with gastrointestinal symptoms. However, the association between cycle threshold (Ct) values from such specimens and the presence of GI manifestations remains unclear.
Materials and methods: An analytical cross-sectional study was conducted using secondary, de-identified hospital records from three Indonesian medical centers (July–November 2020). Adult patients with positive lower GI RT-PCR results and available Ct values were included. Ct values were dichotomized as low (<25) or high (≥25). GI symptoms assessed included nausea, vomiting, abdominal pain, diarrhea, and constipation. The primary outcome was the association between Ct category and the presence of any GI symptom, analyzed using Fisher’s exact test. Results are presented as prevalence ratios (PRs) with 95% confidence intervals (CIs).
Results: A total of 37 patients met the inclusion criteria (43.2% male; mean age 44.8 ± 13.2 years). Only one patient (2.7%) exhibited a low Ct value, while 36 (97.3%) had high Ct values. Overall, 22 patients (59.5%) reported at least one GI symptom. The most frequently reported symptom was nausea (54.1%), followed by vomiting (18.9%), abdominal pain (16.2%), and diarrhea (13.5%); constipation was not observed. No significant association was found between Ct category and the presence of GI symptoms (p = 0.595; PR 1.048, 95% CI 0.956–1.148).
Conclusion: Among adults with SARS-CoV-2 detected via RT-PCR from lower GI specimens, Ct value category was not significantly associated with GI symptom presence. These findings underscore the limited prognostic value of Ct values from lower GI sampling and emphasize the need for larger, prospectively designed studies with standardized protocols.
Wibisono A.M., Fauzi A., Friska D., Suryoadji K.A., Abdullah M., Sudrajat D.G., Surandy A., Muzelina V.N., Syam A.F. Gastrointestinal symptoms and RT-PCR in adults with COVID-19: а post-hoc analysis. The BRICS Health Journal. 2025;2(2):46-51. https://doi.org/10.47093/3034-4700.2025.2.2.46-51
Coronavirus disease (COVID-19) is caused by SARS-CoV-2 and has spread globally since December 2019 [1]. To date, over 6.8 million COVID-19 cases have been reported in Indonesia, with an estimated 162,063 associated deaths1. COVID-19 manifests with respiratory symptoms (e.g., dyspnea) and gastrointestinal (GI) symptoms such as nausea, abdominal pain, and diarrhea [2][3]. The diagnostic gold standard is reverse transcription polymerase chain reaction (RT-PCR) from respiratory specimens – typically nasopharyngeal swabs – but alternative specimens can be informative [2][3]. Wang et al. reported SARS-CoV-2 positivity in fecal specimens of up to 53.4%, and a higher specificity for gastrointestinal symptoms when using lower GI specimens (anal swabs) at approximately 67.5%, compared to nasopharyngeal swabs [4]. Additional studies show high positivity and viral loads in lower GI specimens, detection among asymptomatic cases, and potential reduction in false negatives; anal swabbing may also limit exposure risk for examiners and help pediatric sampling [5][6]. One analytic parameter, the cycle threshold (Ct), inversely reflects viral load and is often used to contextualize RT-PCR results [5][7].
A secondary analysis was conducted using de-identified records from three Indonesian hospitals (RSCM, Mitra Keluarga Depok, and Mitra Keluarga Kelapa Gading) collected between July and November 2020, originally included in Abdullah et al. [3]. Among 136 screened cases, 45 had positive RT-PCR results from lower GI specimens (anal swabs). After excluding 8 records with missing Ct values, 37 participants with complete data were included in the final analysis. This dataset represents all eligible positive cases with Ct information from the three participating centers in the Jakarta region.
GI symptoms captured included diarrhea, constipation, nausea, vomiting, and abdominal pain. Ct values were dichotomized: low <25 vs high ≥25. Categorical variables are presented as the number of patients (n) and the corresponding percentage (%). Age is presented both as a mean with standard deviation and as categorical age groups. Association between Ct category and GI symptom presence was assessed with Fisher’s exact test; effect size is presented as prevalence ratio (PR) with 95% confidence interval (CI). Analyses used SPSS v26. (IBM, the USA).
Participant characteristics (Table 1) showed a near-even sex distribution (43.2% male; 56.8% female) with the majority aged 40–60 years (51.4%), followed by <40 years (37.8%) and >60 years (10.8%). Most patients had no recorded comorbidity (67.6%), while 24.3% had fewer than two and 8.1% had two or more. Obesity (body mass index ≥252) was present in 32.4%. Lifestyle factors included current smoking in 16.2% and former smoking in 8.1%; almost half reported low physical activity and 51.4% reported rarely exercising.
Table 1. Demographic characteristics of participants
Characteristic | Patients, n | Patients, % |
Sex | ||
Male | 16 | 43.2 |
Female | 21 | 56.8 |
Age (years), mean ± standard deviation | 44.8 ± 13.2 | |
< 40 | 14 | 37.8 |
40–60 | 19 | 51.4 |
> 60 | 4 | 10.8 |
Comorbidities | ||
None | 25 | 67.6 |
< 2 | 9 | 24.3 |
≥ 2 | 3 | 8.1 |
Physical activity | ||
Low | 18 | 48.6 |
Rarely (<3/week, <30 min/session) | 19 | 51.4 |
Smoking status | ||
Never | 28 | 75.7 |
Current | 6 | 16.2 |
Former | 3 | 8.1 |
Body mass index (kg/m²) | ||
18.5–24.9 | 25 | 67.6 |
≥ 25 | 12 | 32.4 |
Ct values were predominantly high: 36/37 (97.3%) fell in the high (≥25) category and only 1/37 (2.7%) in the low (<25) category.
GI symptom prevalence was 59.5% (22/37), with 40.5% (15/37) reporting none (Fig). Among symptomatic patients, nausea was most common (12/22), followed by vomiting (4/22), abdominal pain (4/22), and diarrhea (3/22); constipation was not recorded.
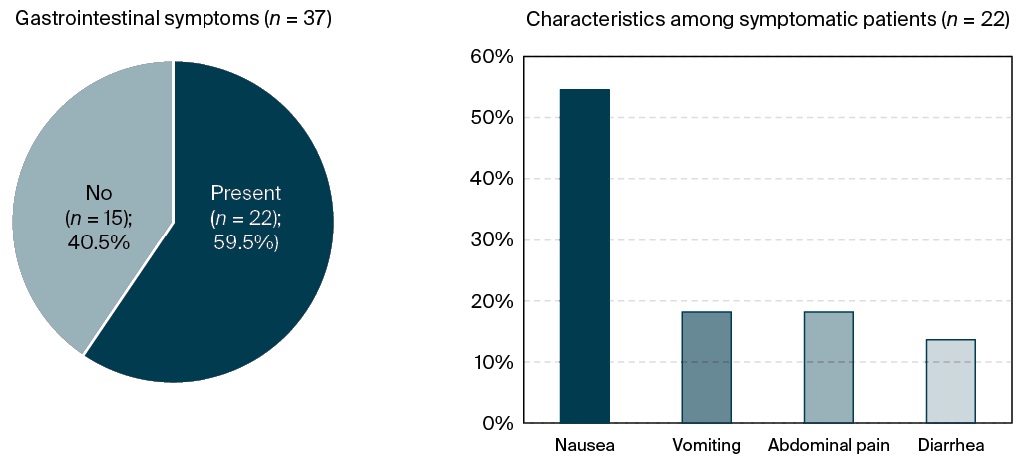
FIG. Prevalence and characteristics of gastrointestinal symptoms
In the primary analysis, the association between Ct category and the presence of any gastrointestinal symptom was evaluated. Due to sparse expected counts, Fisher’s exact test was applied and revealed no statistically significant association (p = 0.595). The prevalence ratio (PR) comparing high versus low Ct values was 1.048 (95% CI: 0.956–1.148), consistent with a null effect estimate (Table 2).
Table 2. Association between cycle threshold category and gastrointestinal symptoms
Gastrointestinal symptoms | Low cycle threshold (n = 1) | High cycle threshold (n = 36) | p-value | Prevalence ratio |
Рresent | 0 (0%) | 15 (41.7%) | 0.595 | 1.048 (0.956–1.148) |
No | 1 (100%) | 21 (58.3%) |
Testing of lower GI specimens serves as a practical complement to nasopharyngeal sampling and has demonstrated higher detection rates in patients with gastrointestinal manifestations, consistent with previous findings from both Indonesian and international studies [3–5][8][9]. Our descriptive data similarly show that GI symptoms were common among adults with positive lower GI specimens RT-PCR.
Despite biologic plausibility that lower Ct (higher viral load) might align with symptomatology, we did not find an association between Ct category and GI symptoms. Ct values are influenced by numerous pre-analytical and analytical factors – including sampling technique, timing relative to illness, transport/storage, and assay efficiency – so crude categorization may obscure clinically meaningful relationships [5][7]. The very low number of low-Ct observations (n = 1) further limits power to detect differences.
Observed heterogeneity in comorbidities and lifestyle risks such as obesity and smoking could also confound relationships between Ct and symptoms, as these factors are associated with COVID-19 outcomes and severity [10]. Future studies should incorporate multivariable adjustments and standardized collection protocols to reduce noise from these sources.
Comparative evidence suggests average Ct values around the high-20s among patients with GI involvement and variable links to severity, yet these patterns originate largely from nasopharyngeal or fecal sampling rather than lower GI specimens [7][9][11]. Standardized, prospective designs that analyze Ct as a continuous measure and align sampling with symptom timing are likely needed to clarify any true association.
In this secondary analysis of 37 adults with positive RT-PCR results from lower GI specimens at three Indonesian hospitals, GI symptoms were common; however, the Ct category (low <25 vs high ≥25) showed no statistically significant association with the presence of GI symptoms (Fisher’s exact p = 0.595; PR 1.048, 95% CI 0.956–1.148). Given substantial pre-analytical variability and potential confounding by comorbidities and lifestyle factors, Ct values from lower GI specimens should be interpreted cautiously for symptom prognostication. Larger, prospective studies with standardized protocols are warranted.
1. Worldometer. COVID Live – Coronavirus Statistics. Accessed 01.08.2025. https://www.worldometers.info/coronavirus/
2. The Asia-Pacific perspective: Redefining obesity and its treatment World Health Organization. Western Pacific Region IASO international association for the study of obesity Accessed 01.08.2025. https://iris.who.int/bitstream/handle/10665/206936/0957708211_eng.pdf?utm_source=chatgpt.com
1. Harapan BN, Harapan T, Theodora L, Anantama NA. From Archipelago to Pandemic Battleground: Unveiling Indonesia’s COVID-19 Crisis. J Epidemiol Glob Health. 2023;13(4):591–603. doi:10.1007/s44197-023-00148-7
2. Goudouris ES. Laboratory diagnosis of COVID-19. J Pediatr (Rio J). 2021;97(1):7–12. doi:10.1016/j.jped.2020.08.001
3. Abdullah M, Sudrajat DG, Muzellina VN, et al. The value of anal swab RT-PCR for COVID-19 diagnosis in adult Indonesian patients. BMJ Open Gastroenterol. 2021;8:e000590. doi:10.1136/bmjgast-2020-000590
4. Wang Y, Chen X, Wang F, et al. Value of anal swabs for SARS-CoV-2 detection: a literature review. Int J Med Sci. 2021;18(11):2389-2393. doi:10.7150/ijms.59382
5. Liu M, Li Q, Zhou J, et al. Value of swab types and collection time on SARS-CoV-2 detection using RT-PCR assay. J Virol Methods. 2020;286:113974. doi:10.1016/j.jviromet.2020.113974
6. Li X, Rong L, Zhang P, Xu J, Rong Y. Significance of nucleic acid-positive anal swabs in COVID-19 patients. Open Med (Wars). 2021;16(1):332-337.
7. Rabaan AA, Tirupathi R, Sule AA, et al. Viral dynamics and RT-PCR Ct values correlation with disease severity in COVID-19. Diagnostics (Basel). 2021;11(6):1091. doi:10.3390/diagnostics11061091
8. Cheung KS, Hung IFN, Chan PPY, et al. Gastrointestinal Manifestations of SARSCoV-2 Infection and Virus Load in Fecal Samples From a Hong Kong Cohort: Systematic Review and Meta-analysis. Gastroenterology. 2020;159(1):81–95. doi:10.1053/j.gastro.2020.03.065
9. Park SK, Lee CW, Park DI, et al. Detection of SARS-CoV-2 in Fecal Samples From Patients With Asymptomatic and Mild COVID-19 in Korea. Clin Gastroenterol Hepatol. 2021;19(7):1387–1394.e2. doi:10.1016/j.cgh.2020.06.005
10. Wolff D, Nee S, Hickey NS, Marschollek M. Risk factors for Covid-19 severity and fatality: a structured literature review. Infection. 2021;49(1):15–28. doi:10.1007/s15010-020-01509-1
11. Taziki Balajelini MH, Rajabi A, Mohammadi M, et al. Virus load and incidence of olfactory, gustatory, respiratory, gastrointestinal disorders in COVID-19 patients: A retrospective cohort study. Clin Otolaryngol. 2021;46(6):1331–1338. doi:10.1111/coa.13844
Andito Mohammad Wibisono, Doctor, Faculty of Medicine
Jl. Salemba Raya No. 6, Kenari, Kec. Senen, Kota Jakarta Pusat, Daerah Khusus Ibukota, Jakarta, 10430
Ahmad Fauzi, Doctor, Faculty of Medicine
Jl. Salemba Raya No. 6, Kenari, Kec. Senen, Kota Jakarta Pusat, Daerah Khusus Ibukota, Jakarta, 10430
Dewi Friska, Staff, Department of Community Medicine
Jl. Salemba Raya No. 6, Kenari, Kec. Senen, Kota Jakarta Pusat, Daerah Khusus Ibukota, Jakarta, 10430
Kemal Akbar Suryoadji, Doctor, Faculty of Medicine
Jl. Salemba Raya No. 6, Kenari, Kec. Senen, Kota Jakarta Pusat, Daerah Khusus Ibukota, Jakarta, 10430
Murdani Abdullah, Professor, Department of Internal Medicine, Division of Gastroenterology, Faculty of Medicine
Jl. Salemba Raya No.6, Kenari, Kec. Senen, Kota Jakarta Pusat, Daerah Khusus Ibukota, Jakarta, 10430
Dedy Gunawanjati Sudrajat, Staff, Department of Internal Medicine, Division of Gastroenterology, Faculty of Medicine
Jl. Salemba Raya No. 6, Kenari, Kec. Senen, Kota Jakarta Pusat, Daerah Khusus Ibukota, Jakarta, 10430
Andry Surandy, Staff, Department of Internal Medicine, Division of Gastroenterology, Faculty of Medicine
Jl. Salemba Raya No.6, Kenari, Kec. Senen, Kota Jakarta Pusat, Daerah Khusus Ibukota, Jakarta, 10430
Virly Nanda Muzelina, Staff, Department of Internal Medicine, Division of Gastroenterology, Faculty of Medicine
Jl. Salemba Raya No. 6, Kenari, Kec. Senen, Kota Jakarta Pusat, Daerah Khusus Ibukota, Jakarta, 10430
Ari Fahrial Syam, Professor, Department of Internal Medicine, Division of Gastroenterology, Faculty of Medicine
Jl. Salemba Raya No. 6, Kenari, Kec. Senen, Kota Jakarta Pusat, Daerah Khusus Ibukota, Jakarta, 10430
Wibisono A.M., Fauzi A., Friska D., Suryoadji K.A., Abdullah M., Sudrajat D.G., Surandy A., Muzelina V.N., Syam A.F. Gastrointestinal symptoms and RT-PCR in adults with COVID-19: а post-hoc analysis. The BRICS Health Journal. 2025;2(2):46-51. https://doi.org/10.47093/3034-4700.2025.2.2.46-51
8/2 Trubetskaya st., Moscow, 119048
Federal State Autonomous Educational Institution of Нigher Education I.M.Sechenov First Moscow State Medical University of the Ministry of Health of the Russian Federation (Sechenovskiy University)
e-mail: bricshealthjournal@staff.sechenov.ru












